Abstract
Legionella pneumophila is the most common cause of atypical pneumonia presenting with rhabdomyolysis. A case is reviewed involving a previously healthy 48-year-old man with Legionnaires’ Disease presenting with a peak CPK level of 1.07 million U/L, the highest degree of elevation that has been reported.
Introduction
Although the association between Legionnaires’ Disease and rhabdomyolysis has been well described in the literature, the degree of creatine phosphokinase (CPK) elevation has not been reported to exceed 462,000 units/liter (U/L) [1]. Here, we present a case of a previously healthy 48-year-old male with Legionnaires’ disease associated with acute kidney injury and severe rhabdomyolysis with a peak CPK of 1.07 million U/L.
Case Presentation
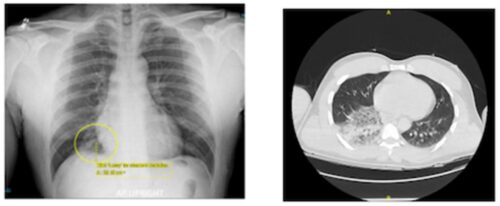
A 48-year-old African American male with no known past medical history presented to the emergency room (ER) with a 3-day history of nausea, vomiting, fevers, and chills. Over the last 48 hours, the patient had developed severe myalgias, especially in his lower back and legs, which prevented him from rising out of bed on the morning of admission. He also admitted to very dark and scant urine production. He denied any respiratory symptoms. The patient was taking no prescription or over the counter medicines and denied any illicit drug use. Upon presentation to the ER, he had a fever to 102 F; he also was tachycardic and tachypneic. His oxygen saturation on room air was 96%. Pertinent laboratory data demonstrated hyponatremia (118 mEq/L), hyperkalemia (5.7 mmol/L), transaminitis (AST 3986 U/L, ALT 1055 U/L), acute kidney injury (serum creatinine of 10.37 mg/dL), and severe rhabdomyolysis with a creatine phosphokinase of 765,000 U/L. An initial chest radiograph suggested a probable developing small right lower lobe pneumonia, which was more pronounced on the chest computerized tomography scan (Figure 1). A further work-up included a negative respiratory viral panel (with negative RSV, Influenza, and COVID-19 PCRs), as well as negative blood cultures. The urine and blood toxicology screens were negative. The patient was started on empiric antibiotic therapy with azithromycin and cefepime, and hemodialysis was emergently initiated. Despite dialysis, the CPK level peaked at 1.07 million U/L. The urine test for legionella Ag returned positive for serogroup 1 on day two after hospital admission. The patient was continued on azithromycin and showed improvement in his symptoms, radiographic findings, and rhabdomyolysis. He no longer required hemodialysis at one month post discharge, as his renal function had normalized.
Discussion
Legionnaires’ disease is a severe multi-system infection with pulmonary, gastrointestinal, musculoskeletal, and neurologic involvement, most often caused by Legionella pneumophila. It is the most common cause of atypical pneumonia presenting with rhabdomyolysis and the second most common cause of serious pneumonia requiring ICU admission [2]. Approximately 30 cases of Legionnaire’ disease presenting with rhabdomyolysis have been previously published in the literature [2], with CPK elevations ranging from 226 U/L to 462,000 U/L [1]. Our patient presented with a CPK of over 1 million U/L, which is the highest reported to date.
The mechanism of legionella-induced rhabdomyolysis has been postulated to arise from either direct invasion of the bacteria into musculature or via the release of a vasoconstrictive endotoxin into the bloodstream, leading to local ischemic damage to myocytes [3]. Sepsis itself could also cause additive muscle injury from fever, rigors, and dehydration [3]. As a consequence, the etiology of acute kidney injury in Legionnaires’ disease may be due to rhabdomyolysis (if presenting with such) as well as acute tubular necrosis (ATN) related to hypotension and hypovolemia from gastrointestinal losses that many patients (including our own) present with [3]. Of note, mortality related to Legionnaires’ disease increases by 40% in those patients presenting with rhabdomyolysis and acute kidney injury [3].
Interestingly, our patient did not present with significant respiratory symptoms but was incidentally found to have pneumonia on a routine chest radiograph performed in the ER. Similar cases of Legionnaires’ disease presenting with extrapulmonary complaints have been reported in the literature, with gastrointestinal issues being the predominant symptomology [4,5]. Our patient did provide an additional history of deep cleaning his basement with a rented power water washer from a local hardware store approximately three days prior to his symptom onset. Given its severe presentation and high mortality rate, Legionnaires’ disease should be considered in patients presenting with gastrointestinal complaints, rhabdomyolysis, and acute kidney injury, especially with the proper epidemiological clues and/or in those with documented pneumonia.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflict of interest.
References
- Hill, J. Incidence and influence of hyperCKemia in legionella infection. J. Neurol. Sci. 2002, 436, 120252. [CrossRef] [PubMed]
- Soni, A.; Peter, A. Established association of legionella with rhabdomyolysis and renal failure: A review of the literature. Respir. Med. Case Rep. 2019, 28, 1–3. [CrossRef] [PubMed]
- Branstetter, A.; Wyler, B. Legionnaires’ disease causing severe rhabdomyolysis and acute renal failure: A case report. Clin. Pract. Cases Emerg. Med. 2022, 6, 288–291. [CrossRef] [PubMed]
- Chennadi, S.; Zulqarnain, S. Legionella: A rare cause of refractory rhabdomyolysis. Chest Inf. 2015, 148, 96–97. [CrossRef]
- Carter, C.J.; Corley, E.M.; Canepa, H.; Schmalzle, S.A. Legionnaires’ disease presenting with exanthem; case and review of previously published cases. ID Cases 2022, 27, e01376. [CrossRef] [PubMed]